by Francis Amèdé, MD
Across the sun-drenched islands of the Caribbean, a quiet health challenge is emerging. While infectious diseases once driven by poverty have largely receded, a new set of health concerns has steadily taken their place.
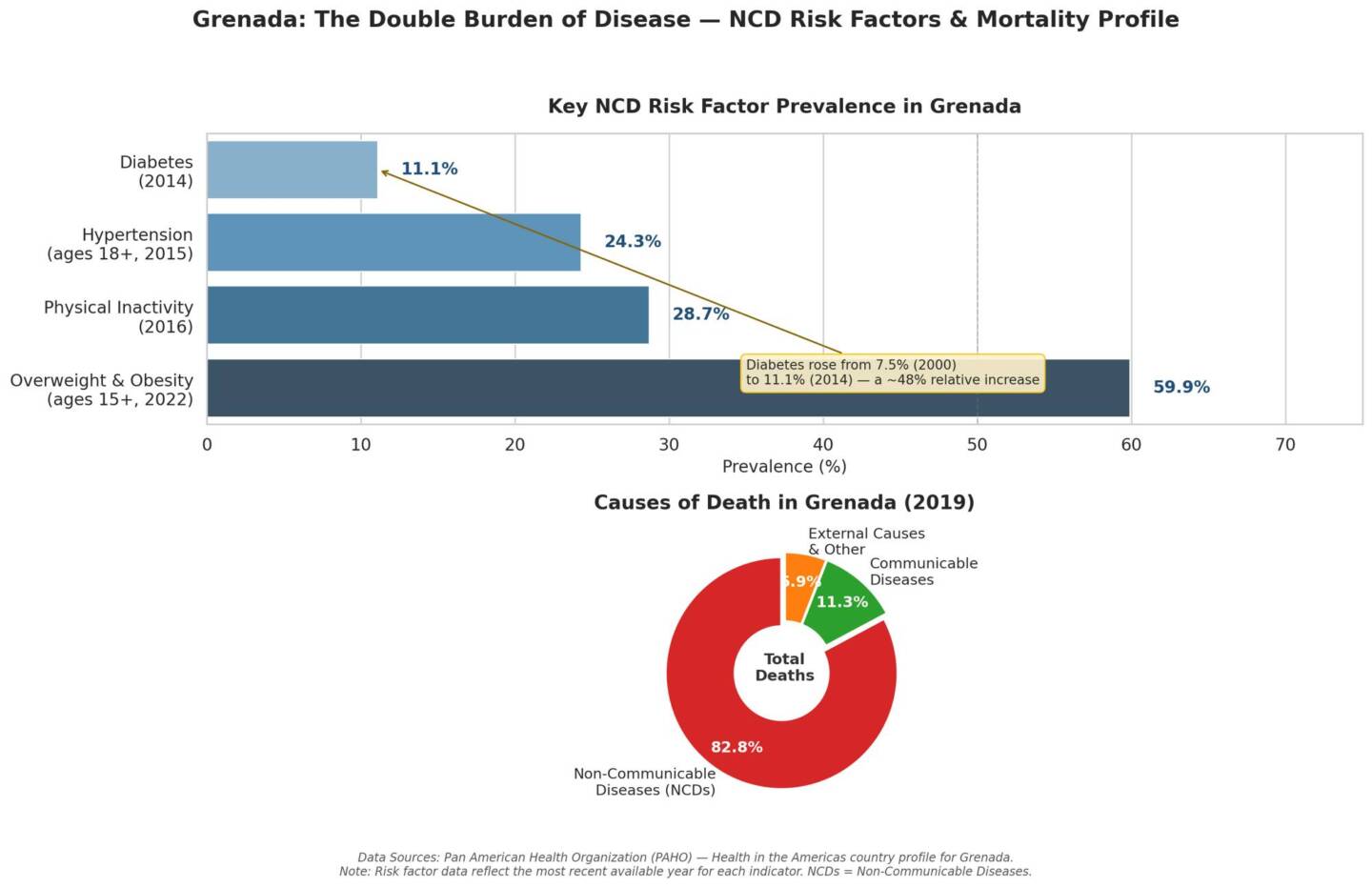
A wave of chronic conditions tied to modern lifestyles has surged. Grenada exemplifies the shift: non-communicable diseases (NCDs) now account for 82.8% of deaths, with cardiovascular diseases, diabetes, and cancers leading the toll. Yet pockets of undernutrition and related vulnerabilities persist, creating a “double burden” that strains families, health systems, and economies.
This is not merely a medical story; it is one of development, inequality, and policy choices. Understanding diseases of affluence versus those of poverty, their overlapping causes, devastating consequences, and proven solutions offers a roadmap. Caribbean governments, particularly Grenada’s Ministry of Health and elected leaders, hold powerful levers for proactive change.
Defining the 2 burdens
Diseases of poverty arise primarily from deprivation: inadequate sanitation, unsafe water, poor housing, limited education, and insufficient nutritious food. They include infectious conditions such as diarrhoeal diseases, respiratory infections, tuberculosis, and HIV, alongside malnutrition (stunting, wasting, micronutrient deficiencies). These illnesses weaken bodies, impair child development, and trap households in cycles of lost productivity and medical debt.
Diseases of affluence or, more accurately today, lifestyle-related NCDs, emerge with economic transition, urbanisation, and changing diets. They encompass obesity, type 2 diabetes, hypertension, cardiovascular disease (heart attacks and strokes), certain cancers, and chronic respiratory conditions. Historically linked to wealthier populations with sedentary jobs, car-dependent transport, and abundant processed foods, these now disproportionately affect lower-income groups within developing societies.
The misleading labels hide a critical reality: in places like Grenada and much of the Caribbean, both burdens coexist. The double burden of malnutrition describes simultaneous undernutrition and overweight/obesity at individual, household, or population levels. Rapid nutrition transitions, driven by cheap imported ultra-processed foods high in sugar, salt, and fat, allow undernourished children to become overweight adults prone to diabetes and heart disease.
In Grenada, data illustrate the scale. Overweight and obesity affect 59.9% of people aged 15 and older (2022). Hypertension prevalence stands at 24.3% among adults 18+ (2015 data), while diabetes rose from 7.5% (2000) to 11.1% (2014). Physical inactivity affects 28.7% (2016). Communicable disease deaths have fallen to about 11.3% of total mortality, yet NCDs claim 82.8%.
 Causes: Structural, Behavioural, and Environmental
Causes: Structural, Behavioural, and Environmental
Poverty-related diseases stem from upstream social determinants: inequitable resource distribution, weak infrastructure, and limited access to care. Overcrowding and poor water/sanitation fuel infections; food insecurity drives malnutrition.
Affluence-related diseases trace to the Westernisation of diets and lifestyles. Urbanisation reduces physical activity. Motorisation and desk jobs replace walking and manual labour. Globalised food systems flood markets with inexpensive, energy-dense processed items while fresh local produce becomes relatively costlier or less available. Aggressive marketing, especially to children, normalises sugary drinks and snacks. Tobacco and alcohol use compound risks. Stress from economic pressures and longer lifespans (with cumulative exposure to risks) amplify chronic disease.
Critically, the poor often bear the brunt of both. Cheap calories from processed foods drive obesity among low-income families, while undernutrition lingers in early life or rural pockets. This creates a vicious intergenerational cycle: early stunting raises later obesity and NCD risk. In the Caribbean, high food import dependence, tourism-driven economies, and climate vulnerabilities accelerate these shifts. Historical successes against infectious diseases (vaccination, basic sanitation) have lengthened lives, only for NCDs to emerge as the new killers.
Consequences: Human suffering and economic drag
The human cost is staggering. NCDs cause premature death (before age 70) and years lived with disability. In low and middle-income countries, 82% of premature NCD deaths occur. Cardiovascular disease alone drives massive mortality. Diabetes leads to kidney failure, blindness, and amputations. Obesity fuels joint disease, sleep apnea, and mental health burdens. Poverty diseases still exact a toll through child mortality, lost schooling, and weakened workforces, perpetuating inequality.
Economically, the burden is unsustainable. Caribbean NCDs cost between 1.36% and 8% of GDP in direct healthcare and indirect productivity losses across countries, figures that exclude broader societal impacts. In Grenada and its neighbours, hospital discharges for chronic illness are dominated by cardiovascular conditions. Families face catastrophic out-of-pocket expenses; governments divert resources from education or infrastructure. Lost workdays from illness and caregiving reduce national output. The double burden compounds this: stunted children become less productive adults, while NCDs strike working-age populations hardest.
Societally, these diseases widen health inequities. Women, rural residents, and lower-income groups often face compounded risks and poorer access to screening or treatment. Health systems designed for acute infections struggle with lifelong chronic care needs.
Concrete, evidence-based solutions
Effective responses exist and are cost-effective. The World Health Organisation’s updated best buys and recommended interventions target the 4 main NCD risk factors, tobacco, alcohol, unhealthy diet, and physical inactivity, plus clinical management.
For NCDs (diseases of affluence)
- Fiscal measures: Increase taxes on tobacco, alcohol, and sugar-sweetened beverages (SSBs). Grenada’s 2023 implementation of raising VAT on sweetened beverages to 20% is a strong start; rigorous evaluation and expansion can amplify impact
- Regulation: Front-of-pack nutrition labelling (inspired by successful models elsewhere), restrictions on marketing unhealthy foods to children, and reformulation targets for salt, sugar, and trans fats in local products
- Environment and behaviour: Create walkable communities, subsidise or promote fruits and vegetables, integrate physical activity into schools and workplaces, and scale community exercise programmes
- Clinical best buys: Systematic cardiovascular risk assessment and management (e.g., hypertension and diabetes control), plus secondary prevention
For diseases of poverty and the double burden
- Strengthen water, sanitation, and hygiene (WASH)
- Scale proven nutrition interventions: Exclusive breastfeeding promotion, complementary feeding support, micronutrient supplementation, and deworming
- Double-duty actions: Integrate obesity prevention into existing undernutrition programmes (e.g., counselling on responsive feeding that avoids overfeeding)
- Universal health coverage with strong primary care for early detection and integrated management
Cross-cutting: Robust surveillance, multisectoral action plans, and health-in-all-policies approaches. Community health workers can deliver education, screening, and support, especially in underserved areas.
Educating the public for sustainable change
Knowledge alone does not change behaviour, but well-designed applied education does. Mass media campaigns using local languages, storytelling, and trusted figures (doctors, athletes, pastors, calypsonians) can shift norms around diet, activity, and substance use. School curricula must embed nutrition literacy, practical cooking skills, and daily physical activity from early ages.
Community-level efforts, via health centres, churches, youth groups, and markets, build skills and social support. Point-of-purchase labelling and digital tools (apps, SMS reminders) empower individuals. Campaigns should address myths (e.g., healthy food is too expensive) with practical, affordable Caribbean recipes using local produce. Evaluation is essential: track knowledge, attitudes, and ultimately risk factor changes.
Public education works best when paired with environmental changes that make healthy choices easier and default options.
The proactive role of Caribbean Governments and ministers for health
Elected representatives, especially ministers for health, cannot treat this as a downstream clinical problem. They must lead upstream prevention with urgency and coordination.
Grenada’s recent progress, achieving national scale-up of the PAHO HEARTS initiative for standardised hypertension and diabetes care, demonstrates what is possible. Building on the 2013 National Chronic Non-Communicable Disease Policy and Multisectoral Action Plan, leaders should:
- Update and fully fund national NCD and nutrition strategies with clear targets aligned to Sustainable Development Goal 3.4 (reduce premature NCD mortality by one-third by 2030)
- Champion legislation and fiscal policy: Expand and enforce SSB taxation, implement front-of-pack labelling, restrict unhealthy food marketing to children, and create healthy public food procurement policies (schools, hospitals, government offices)
- Drive multisectoral governance: Establish or revitalise high-level NCD commissions involving Finance (for taxes), Agriculture and Trade (food systems), Education (schools), Sports and Youth, Urban Planning, and civil society. Health must sit at the cabinet table for all major policies
- Invest in primary care and integration: Scale HEARTS and similar models, train community health workers, ensure essential medicines and technologies are available and affordable, and link NCD services with maternal/child health and nutrition programmes for double-duty impact
- Strengthen data and accountability: Improve surveillance using PAHO/WHO tools, publish regular progress dashboards, and conduct operational research on what works locally
- Address social determinants: Collaborate on poverty reduction, food security, housing, and education equity, recognising that healthier populations drive economic growth
Foster regional solidarity: Work through Caricom, PAHO, and Caribbean Public Health Agency (CARPHA), the regional public health organisation serving Caribbean Community (Caricom) member states. It coordinates disease surveillance, health research, laboratory services, and public health responses across the Caribbean region for joint procurement, shared learning, and harmonised standards (e.g., labelling, marketing rules). Learn from neighbours’ pilots, such as performance-based financing in Saint Lucia.
Ministers must also model and champion prevention publicly, allocate budgets proportionally to prevention (often dwarfed by curative care), and resist industry interference. Proactive leadership means acting before crises peak, investing today saves lives and money tomorrow. Evidence shows every dollar spent on proven NCD prevention yields substantial returns in health and productivity.
A call to integrated action
Grenada and the Caribbean stand at the crossroads. The diseases of poverty are not fully vanquished, and those of affluence now dominate, yet the tools to address both exist. By tackling root causes through multisectoral policy, empowering communities with education, and investing in prevention within strong primary care systems, leaders can bend the curve.
The human and economic stakes could not be higher. With political will, evidence-based applied action, and genuine partnership across government, civil society, and citizens, the Caribbean can transform this double burden into a story of resilience and renewed health successes for generations to come.