






We listened carefully to concerns expressed in response to the Government’s proposed Age of Civil Legal Responsibility (Amendment) Bill.
Last September, we prepared recommendations designed to address those concerns and others intended to strengthen the Bill. We would like to share our recommendations.
We proposed that 2 basic norms be required of health professions and must be explicit in training those dealing with adolescents:
- they routinely explore the prospect of parental involvement, and
- they inquire about the willingness of the adolescent to report any undesirable situation. They should act only on the adolescent’s expressed consent
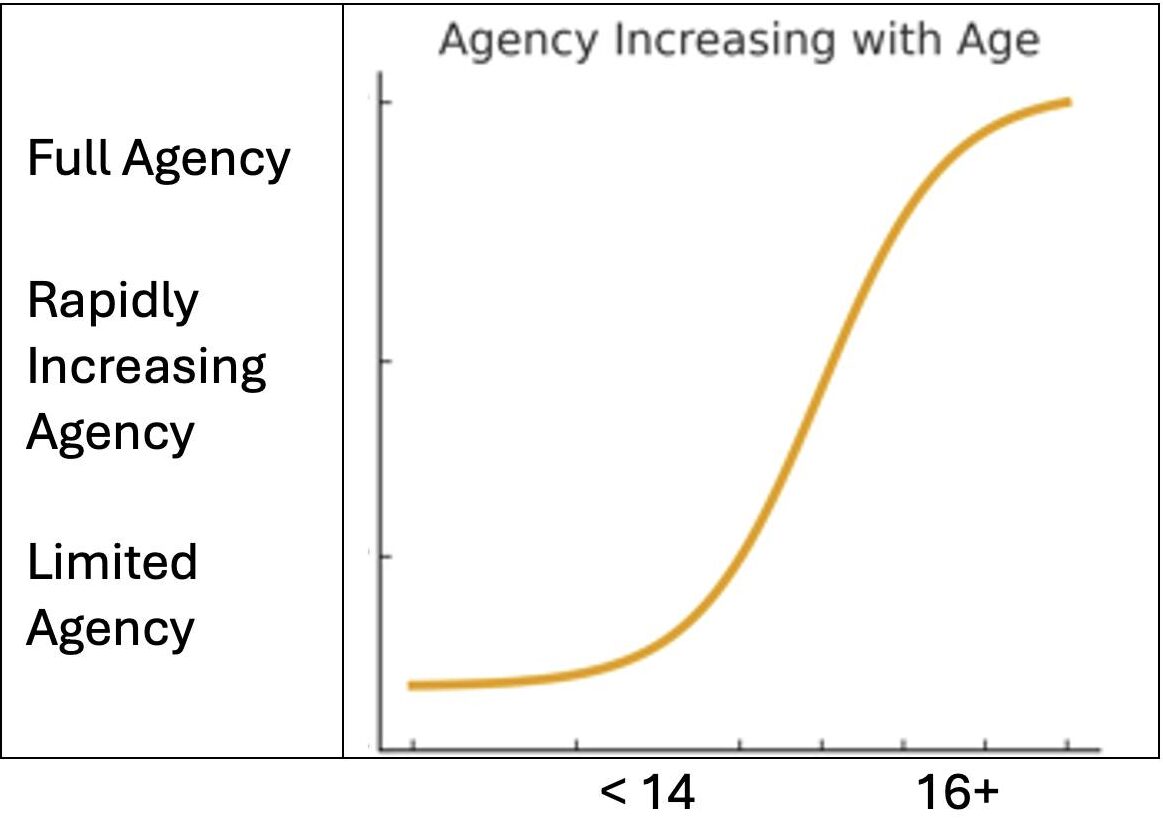
Our recommendations are framed in the context of the evolving capacity of adolescents. We can consider this visually in the form of a sigmoid curve. The x-axis depicts increasing age, and the y-axis shows increasing agency. We propose different approaches for older adolescents 16+, those 14–15, and those under 14.
For 16–17-year-olds
For adolescents 16–17 years old, we recommend full autonomy as currently proposed.
Our only qualification for this group is that if such an adolescent has an impairment that clearly affects their decision-making, then in those exceptional circumstances, the health professional should seek the involvement of an adult third party. Ideally, this would be a parent, if appropriate. If not, another adult relative, an officer from the state’s support services, or a relevant non-governmental organisation. In all other cases 16 and 17-year-olds should be treated as today’s 18-year-olds.
14–15-year-olds
We recommend extending access to 14– and 15-year-olds with further qualifications. For this group, the overarching norms of parental/adult involvement and reporting with the minor’s consent also apply.
We recommend adopting the Gillick standard and Fraser guidelines as further instruments for health professionals. The key element here is the removal of the current legal prohibition on healthcare workers and instead replacing it with a reliance on their judgement and professionalism.
We recommend establishing guidelines about the range of services that will normally be provided to this group without parental knowledge or consent, and which ones will not be provided without parental engagement, or the involvement of some other adult relative, or an appropriate state or non-governmental organisation.
Below 14
We recommend extending access to adolescents below the age of 14. The services to this group would be even more limited. Adult engagement would be required, although not necessarily a parent. For this group, the dominant emphasis would be information and education. The adult chosen should be with careful regard to the best interest of the child.
As with the 14–15 group, there should be guidelines on what services would be routinely provided and which ones would require parental engagement, if appropriate or some other trusted adult.
There is a clear need to reach this younger group through Health and Family Life Education (HFLE) programmes in schools. This will not be a quick fix. It will involve training teachers and ensuring their comfort with the material. It will almost certainly involve collaboration between the Ministry of Education and the Ministry of Health, and if the curriculum is to be age-appropriate, considerable consultation with parents will be essential in formulating it. Fortunately, HFLE already exists in most schools.
Successful adulthood does not suddenly bloom on one’s 18th birthday, or the need for SRH information and services on the 16th. The programme we have outlined is one that facilitates and nurtures the gradual growth toward adult agency.
The operation of the law
So much for the substance of the law. Equally important in the context of a law that has aroused such intense debate is the processes that guide its operation.
We therefore urged the Government to prepare regulations simultaneously with revision and deliberation of the Bill. The law is one thing; giving muscle to the law through regulations is another. Mindful of the intense public discourse, we implored the Government to establish:
- Procedures for outreach to parents, teachers and religious leaders
- Guidelines for orienting health professionals working with adolescents
- Norms and procedures along the lines of the three age groups proposed earlier, for example, criteria along the Gillick standard (Scarman) or Fraser tests
- For those under 16, procedure for strengthening sexuality education
- Guidelines for the appointment of a non-governmental body to advise the Minister on securing the effective operation of the Amendment
- Guidelines for strengthening parental engagement in sexual discourse and so ending the cultural silence in these matters, and
- A basic anonymous reporting form for tracking SRH services to adolescents
We believe that creating a non-governmental oversight body would be a powerful signal of commitment to transparency and accountability. Given the intensity of the public debate about the Bill, such a platform could go a long way in quenching anxiety, building trust, and monitoring the improvement in adolescent sexual health.
Sincerely,
Tonia Frame, President, Grenada Planned Parenthood Association (GPPA)
Fred Nunes, Consultant, Advocates for Safe Parenthood: Improving Reproductive Equity (ASPIRE)